DOSISPHERE-01 overview
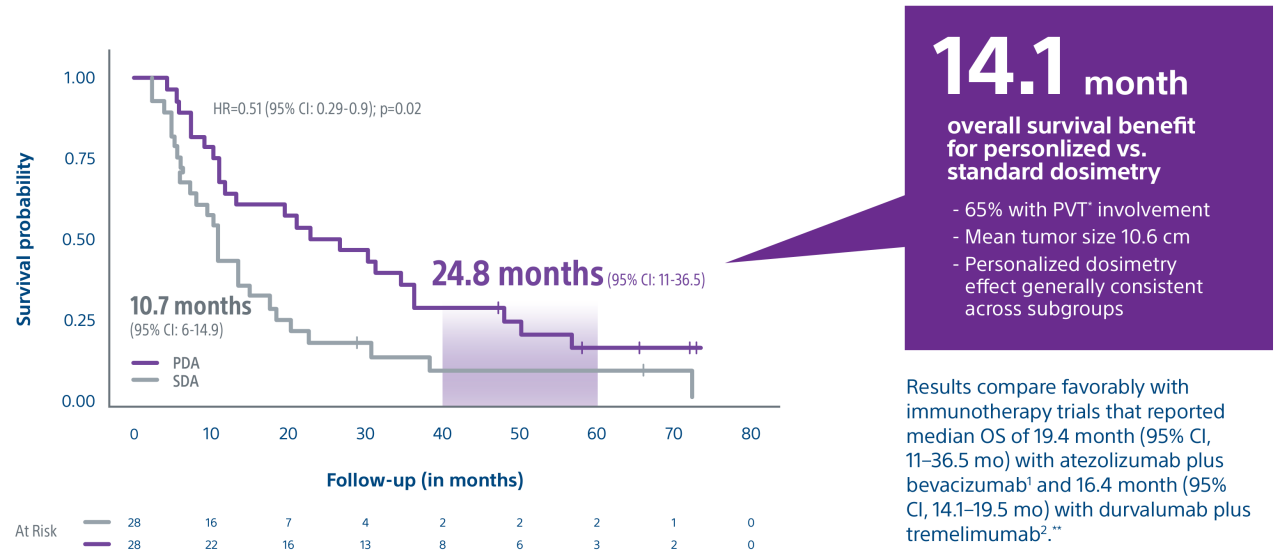
Phase 2 randomized trial showed that advanced HCC patients who received a personalized TheraSphere dose using multicompartment dosimetry had a median OS of 26.6 months, a 16-month improvement compared to the control arm.
Garin E, Tselikas L, Guiu B et al. Personalized versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): a randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol Hepatol. 2021, 6: 17-29
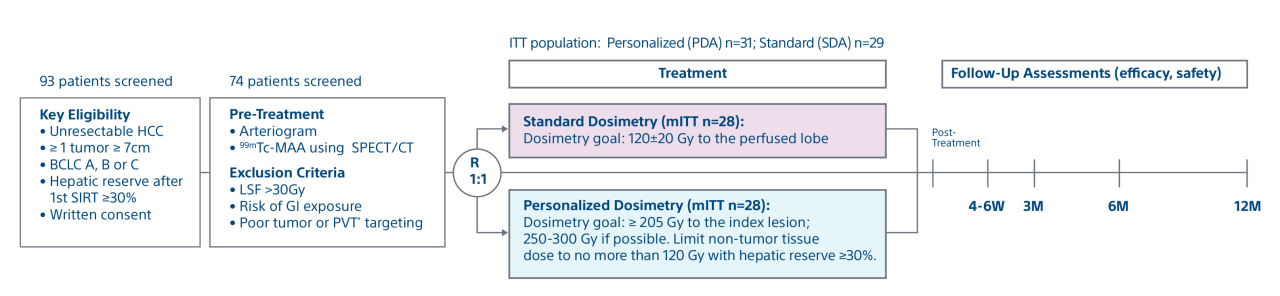
Study objective and design
A randomized, multicenter, investigator sponsored phase II trial comparing the clinical outcomes of SIRT with TheraSphere in patients with intermediate/advanced HCC using two pre-treatment dosimetry determination methods: (1) Standard, single-compartment dosimetry (SDA); defined as a uniform distribution of absorbed dose within the perfused volume – both tumor and normal liver or (2) Personalized dosimetry (PDA); defined as multi-compartment Y-90 distribution of absorbed dose within the perfused volume that accounts for preferential blood flow into the tumor compared with normal parenchyma.