EMBLEM™ MRI S-ICD System
Subcutaneous Implantable Defibrillator
ATLAS Randomized Controlled Trial: S-ICD Superior to TV-ICD1
Study overview
The ATLAS Trial is an investigator-sponsored research study (ISR) initiated, designed and led by Population Health Research Institute (PHRI), Jeff S. Healey MD, MSc, FHRS, and the ATLAS Steering Committee. It is the first prospective randomized controlled trial where the primary objective was to evaluate lead-related complication rates between the S-ICD and single chamber TV-ICD devices at six months after implant.
Hypothesis
The trial hypothesis is that S-ICD is superior to TV-ICD with respect to serious lead-related complications*, including:
- Moderate-severe or severe tricuspid regurgitation
- Hemothorax or pneumothorax
- Cardiac perforation, tamponade, or pericardial effusion or pericarditis
- Ipsilateral upper extremity deep vein thrombosis
- Lead dislodgement or loss of sensing or pacing requiring revision
Sample Size and Timing
The trial randomized 503 patients, who passed electrocardiographic screening, from clinical centers across Canada between February 2017 and July 2021.

Primary Outcomes
Patients in the S-ICD group showed significantly fewer serious lead-related complications* than patients implanted with a single-chamber TV-ICD.


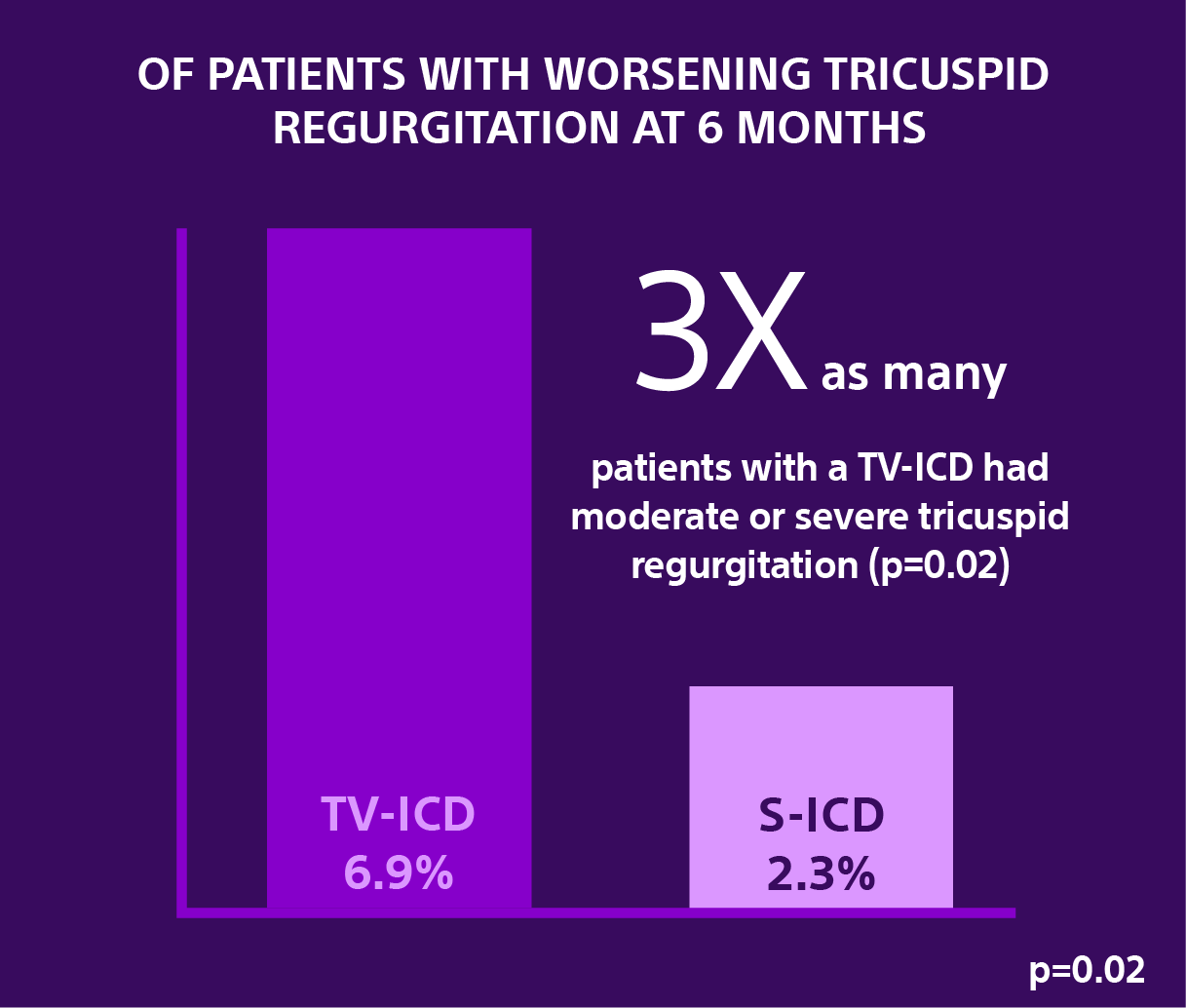
Secondary Analysis: Effects of Implantable Cardioverter-Defibrillator Leads on the Tricuspid Valve and Right Ventricle: A Randomized Comparison of Transvenous versus Subcutaneous Leads.24
Data from a secondary analysis of the investigator-sponsored research ATLAS trial evaluated in nearly 450 patients the severity of Tricuspid Regurgitation (TR) at six months following the implantation of a transvenous implantable cardioverter-defibrillator (TV-ICD) versus the EMBLEM S-ICD.

PRAETORIAN: S-ICD vs. TV-ICD
First results of the randomized PRAETORIAN-DFT trial
Prospective validation of the PRAETORIAN score for prediction of defibrillation test success after subcutaneous ICD implant
The findings from this first analysis demonstrate that a low (<90) PRAETORIAN score is 99% predictive for a successful DFT and a high (≥90) PRAETORIAN score is the strongest predictor for DFT-failure (odds ratio of 34 ).25
While the study investigators concluded their presentation by stating that the PRAETORIAN score could be used as an alternative for DFT in cases when DFT-testing is not possible or desirable, omitting DFT’s in S-ICD implants cannot be advised until the full PRAETORIAN-DFT results are available.
Analysis of the UNTOUCHED Study
Hypothesis
The incidence of inappropriate shocks in primary prevention, LVEF ≤ 35% patients will be non-inferior to the rate in transvenous ICD patients with similar programming observed in MADIT-RIT Arms B and C.
Study Design
- Follow-up for 18 months
- Device programming with a conditional zone of 200 bpm and a shock zone of 250 bpm
- Primary endpoint of inappropriate shock-free rate at 18 months
- Secondary endpoints of all cause shock-free rate at 18 months and system and procedure complications at 30 days
Key Takeaways
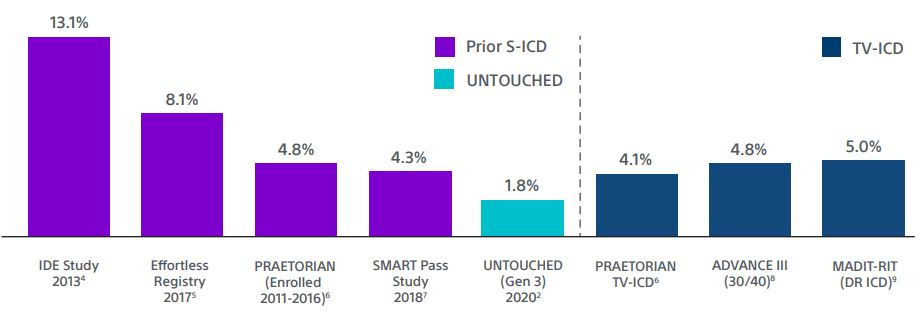
1. The inappropriate shock rate of 2.4% at 1 year for EMBLEM™ MRI S-ICDs is the lowest reported for S-ICD, despite a cohort with more left ventricular dysfunction and heart failure.2
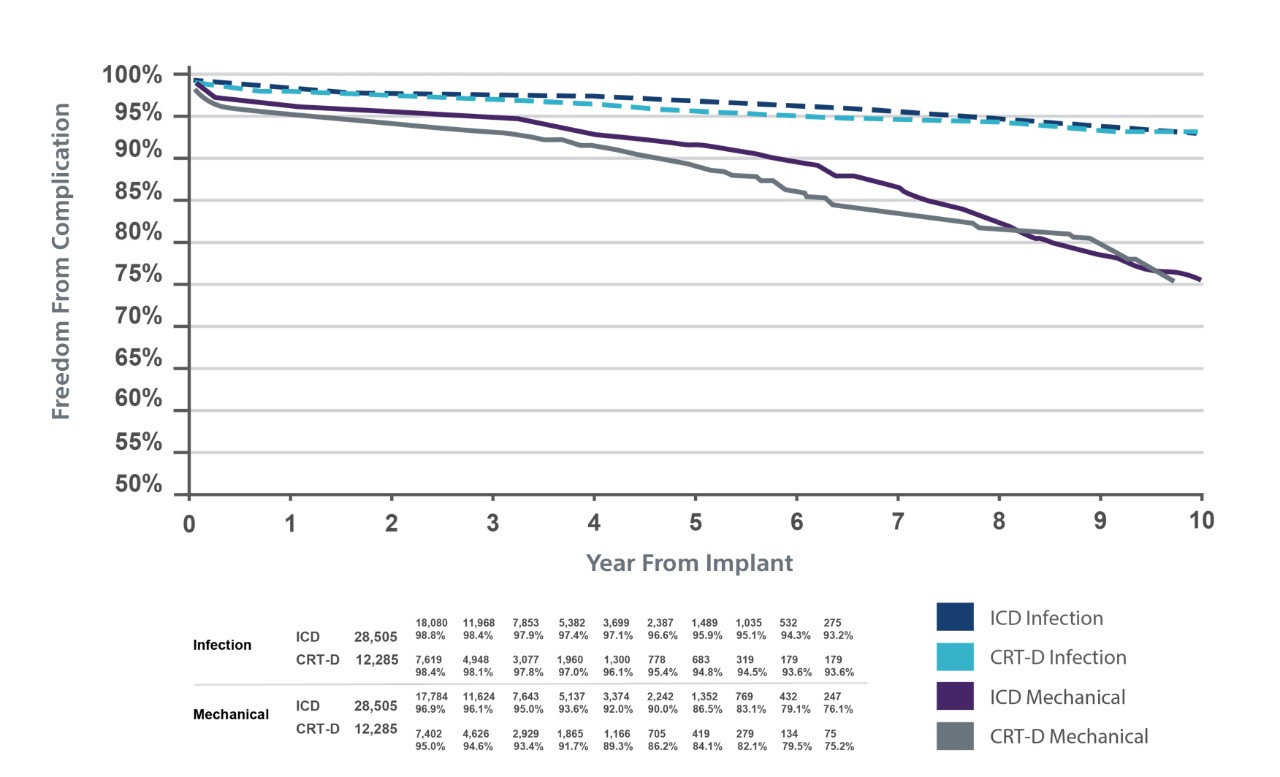
TV-ICD Lead Complications in the Real World



S-ICD is Guideline Recommended




Analysis of MADIT RIT Data22
A new analysis of data from MADIT RIT demonstrates patients are more likely to develop complications from transvenous leads than they are to benefit from ATP.
- There is a statistically significant reduction in ATP with contemporary programming, suggesting that many VTs are self-terminating and earlier interventions may lead to an overestimation of the value of ATP.
- Despite the use of significantly more ATP in the conventional programming arm of MADIT RIT, there was no reduction in the final shock rate when compared to the contemporary programming arms.

SMART Pass Significantly Reduces IAS

Clinical Data Resources
Dr. Michael Gold Discusses the UNTOUCHED Study at HRS 2020
The Impact of SMART Pass on IAS
S-ICD and Patients at High Risk for Infection
Training & Education

Explore continuing education courses, best practices modules and other training and resources for S-ICD.
Why S-ICD?
See how S-ICD helps protect patients at risk for sudden cardiac death while also eliminating the risk of TV-ICD lead complications.

Implant Procedure
Learn about advancements in the S-ICD implant procedure, including the 2-incision and intermuscular implant techniques.
Videos & Resources
Hear physician perspectives about S-ICD, find media information, and download product images, patient videos and more.